With 2024 closing on calls to strip medicinal cannabis from the Special Access Scheme, Andrew Proudfoot argues the industry has no choice but to mount a strong defence in 2025.
The head of the Therapeutic Goods Administration (TGA) recently went on record defending prompt access to medicinal cannabis for Australians with unmet clinical needs where approved treatment options are limited or absent. The fact that he felt compelled to do so says something about where this debate currently stands.
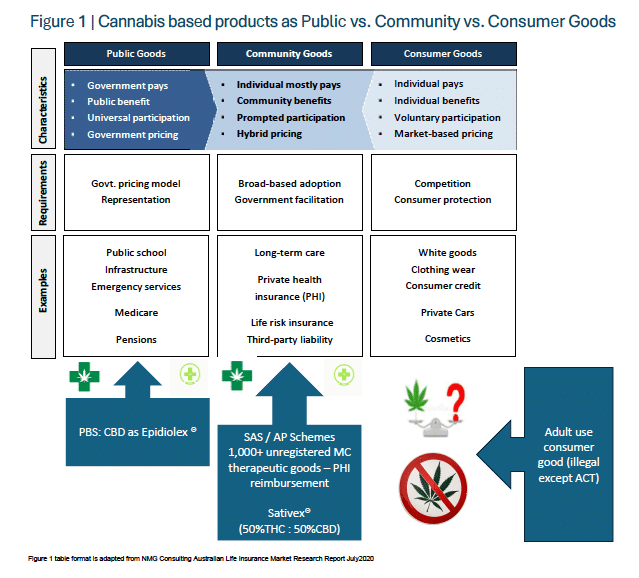
Cannabis occupies an unusually complicated position in Australia. Depending on how it is obtained and where in the country you live, the same plant can simultaneously be a legal medicine serving the public good, a community good, or an illicit consumer product. It remains a political and medical punching bag — a legacy of decades of prohibition. In practice, cannabis exists across several distinct regulatory categories:
- A specialist-supervised, PBS-listed medicine prescribed as 100% cannabidiol (Epidiolex), which has cleared the threshold of a genuine public good — meaning evidence conclusively supports its therapeutic value and taxpayers subsidise its use as adjunctive therapy for seizures linked to Lennox-Gastaut syndrome.
- An Australian Register of Therapeutic Goods (ARTG)-approved community good in the form of a 50:50 THC/CBD prescription sublingual spray (nabiximols/Sativex) for intractable pain and muscle spasticity in multiple sclerosis.
- Broadly, a community good — the roughly 1,000 preparations regulated and accessed as unregistered medicines under the Special Access Scheme (SAS) or Authorised Prescriber (AP) scheme, available in varying ratios and forms.
- An illicit drug, or a legally home-cultivated adult-use product if you happen to live in the Australian Capital Territory — but nowhere else in the country.
When something earns public good status, governments respond with pricing and subsidy models like the PBS, as seen with Epidiolex, to maximise benefit for a proven indication.
Products containing THC have not reached that threshold in most eyes, and so they remain largely in community good territory.
Community goods are defined, in part, by who bears the cost of access. Eight years on from the legalisation of medicinal cannabis in Australia, not one of the approximately 1,000 available products has achieved ARTG registration, and further PBS listings remain a distant prospect.
Four years after low-dose CBD was down scheduled, the TGA has yet to approve any product entries, which means affordable and timely access to medicinal cannabis continues to be shaped by market forces operating within the SAS and AP pathways — channels that remain critical for patients and prescribing practitioners alike.
Private health insurers have begun partially reimbursing the cost of medicinal cannabis prescriptions, though pharmaceutical cover limits vary considerably. Out-of-pocket expenses for cannabis-based treatments and non-Medicare-subsidised consultations remain common.
Adding to the complexity, many practitioners registered with the Australian Health Practitioner Regulation Agency (AHPRA) have received no training on the endocannabinoid system — a key homeostatic regulator of numerous physiological processes and neuromodulatory activity in humans — or on the plant-derived cannabinoids used to interact with it.
This gap in training leaves many clinicians sceptical about the quality of evidence underpinning medicinal cannabis in professional practice.
Despite that, more than 5,500 Australian doctors have written prescriptions for the medicine, and over one million scripts have been approved through TGA pathways.
The absence of so-called gold-standard clinical trial data required for formal ARTG registration across these roughly 1,000 products does not mean there is no evidence of efficacy, safety or tolerability for practitioners to draw on when making prescribing decisions.

If cannabinoids demonstrably reduce the overall burden of disease — through lower pain levels and reduced healthcare costs, less absenteeism, or improved social and economic participation including gains in work capacity and health-related quality of life — and if they are generally safe, well tolerated and efficacious based on real-world data, then restricting access on largely theoretical grounds does not serve the public interest.
That said, the contested nature of the evidence leaves patients, practitioners and the broader sector exposed to criticism.
In November, Queensland representatives from the AMA, the Royal Australian and New Zealand College of Psychiatrists (RANZCP) and the Pharmacy Guild of Australia jointly wrote to the TGA expressing what they described as "serious concern" and "alarm" over what they characterised as high-volume prescribing of unregistered, high-THC medicinal cannabis products in the state.
The letter alleged that medicinal cannabis dispensed under the SAS was contributing to inappropriate use, and the authors recommended it be removed from the scheme and regulated like all other drugs of dependence.
Then in December, the Medicinal Cannabis Expert Working Group released an update on an ongoing study examining the health impacts of high-potency, category 5 THC products available under the SAS and AP scheme, focusing on their efficacy and safety profile.
These developments, together with heightened AHPRA enforcement activity, point to the ongoing difficulty of balancing the regulatory, political and medical legitimacy of cannabis in Australia — particularly when it comes to high-THC preparations.
What did the AMA, RANZCP and Pharmacy Guild allege?
Among other claims, the joint authors:
- Claimed the TGA's standards for regulating medicinal cannabis products and their THC concentrations were inadequate.
- Claimed patients, particularly those with psychotic illnesses, are suffering significant adverse health outcomes from inappropriate prescribing and use of products with high concentrations of THC.
- Urged the TGA to provide more information to health practitioners about appropriate prescribing, and called for better regulation, particularly regarding the concentrations of THC allowable under relevant legislation.
- Signalled their alarm that high-THC products "continue to be prescribed for conditions for which there is no evidence, including anxiety, insomnia and chronic pain and for patients with comorbidities or who are taking other medicines where use of medicinal cannabis is contraindicated".
How did the TGA respond, and what does that signal to the broader community?
Confirming that medicinal cannabis is a priority area for the regulator, TGA chief Professor Anthony Lawler acknowledged "the importance of timely access to unregistered therapeutic goods to address the medical needs of patients, in clinical circumstances where there are limited or no approved treatment options".
He added: "The prescribing of an unregistered medicinal cannabis product through the Special Access Scheme, as with any unregistered therapeutic good, requires the prescribing clinician to comply with good medical practice, the principles that characterise ethical and professional conduct expected of doctors by their professional peers and the community."
Pushing back against the letter's authors, he stated: "Regarding the provision of clinical guidance for medical practitioners, it is important to note that the development of clinical guidance is generally outside the remit of the TGA.
"It would be highly valuable for best-practice clinical resources to be led by expert peak medical and pharmacy bodies with the relevant expertise in conditions where medicinal cannabis is being prescribed in high volumes, such as for the management of chronic pain and anxiety. This would include the relevant medical colleges." [my emphasis]
What does this reveal about peak medical and pharmacy bodies and their role in cannabis regulation?
The TGA already carries a heavy workload evaluating, assessing and monitoring therapeutic goods — including medicinal cannabis — without being drawn into responding to the poorly grounded concerns of peak bodies.
While the Department of Health, via the TGA, put in place baseline guidance for patients and practitioners back in 2017, it falls to the Australian Medical Council and specialist colleges and health professional bodies to update accreditation standards, training programs and clinical guidelines relating to medicinal cannabis.
They have ignored the 2020 Senate report that called on them to do exactly that, and in doing so have placed both patients and their own members in an untenable position.
The National Library of Medicine/PubMed website holds more than 49,500 scientific papers on cannabis going back to 1840. There is reasonable quality evidence for the efficacy and safety of medicinal cannabis in treating anxiety, insomnia and chronic pain, including for the use of high-THC preparations in certain of these indications.
When the peak body co-authors told the TGA that no such evidence exists, they put forward a position that is objectively false and contributes nothing useful to scientific, political or legal debate about cannabis's place in Australian society.
Some recent examples from the higher-quality, evidence-based literature on cannabis for anxiety, insomnia and chronic pain — readily available to the community and to the peak bodies — can be found at the following links:
https://www.dea.gov/sites/default/files/2024-05/2016-17954-HHS.pdf
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0272241
https://pmc.ncbi.nlm.nih.gov/articles/PMC10998028
https://www.bmj.com/content/382/bmj-2022-072348
Where does this leave the industry?
Every Australian has the right to the highest attainable standard of physical and mental health, along with access to the facilities, goods, services and conditions needed to achieve it — and that includes access to medicinal cannabis.
Cannabis is a community good. Calling for it to be stripped from the SAS and treated the same as all other drugs of dependence would deprive Australians of medicines that access to good health — a human right — demands they be able to obtain.
The joint peak body letter reflects a disregard for community goods and human rights alike, and reveals more about the organisations' failure to update their own training and quality standards than it does about the TGA, therapeutic goods regulation or the medicinal cannabis sector.
The campaign against THC prescribing in Australia continues — and it is being driven, troublingly, by the very medical and pharmacy bodies charged with helping Australians maintain their physical and mental wellbeing.
In the meantime, medicinal cannabis advocates need to publicly defend and reinforce to the Department of Health, medical bodies and the community some basic key messages in 2025 to fight back in this ongoing war:
- Medicinal cannabis access — inclusive of THC — is a community good.
- While there are legitimate concerns about the prescribing of high-THC products, access must be timely and not unduly restrictive, including to category 5 medicine.
- THC can help address the medical needs of Australians, in clinical circumstances where there are limited or no other approved treatment options, such as for chronic pain, anxiety, insomnia and other conditions.
Andrew Proudfoot is an Australian solicitor and financial planner specialising in tax, insurance, and commercial law and has acted on TGA advertising and business sale matters involving medical cannabis.
He is also a part-time MPhil candidate at NICM Health Research Institute, Western Sydney University and has published on endometriosis, cannabinoids and insurance medicine in ANZJOG and Nature, Drugs.
He writes here in a private capacity and his views do not represent those of the organisations he is licensed or employed with, or that he advises/consults to.


